


Staged Tendon Reconstruction
Staged tendon reconstructions are indicated for delayed or neglected flexor tendon injuries and tendon rupture following previous attempted repair if the fibro-osseous tunnel has significantly contracted and is not amenable to primary tendon grafting. It is contraindicated in isolated flexor digitorum profundus (FDP) injuries with an intact flexor digitorum superficialis (FDS) as attempted reconstruction of the FDP may result in worse digital flexion function and in such cases tenodesis of the FDP or distal inter-phalangeal joint fusion (arthrodesis) should be performed instead. A supple digit with full passive flexion is essential prior to any attempt at flexor tendon reconstruction.
 Resting posture showing loss of the normal flexion cascade of the ring and little fingers
Resting posture showing loss of the normal flexion cascade of the ring and little fingers
 Flexion attempted revealing absent flexion of the ring and little fingers.
Flexion attempted revealing absent flexion of the ring and little fingers.
 Dorsal view of attempted flexion.
Dorsal view of attempted flexion.
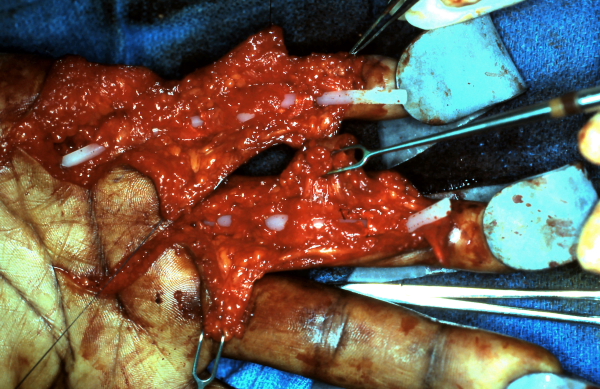 Ring and little fingers with the flexor tendons excised and silicone tendon spacers in place. Care taken to minimize damage to the flexor sheath in particular the A-2 and A-4 pulleys.
Ring and little fingers with the flexor tendons excised and silicone tendon spacers in place. Care taken to minimize damage to the flexor sheath in particular the A-2 and A-4 pulleys.
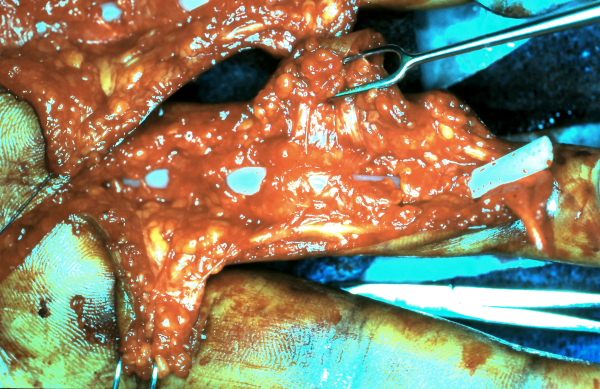 Close up view.
Close up view.
 Full passive flexion must be obtained post operatively before the second stage and tendon grafting can be performed.
Full passive flexion must be obtained post operatively before the second stage and tendon grafting can be performed.
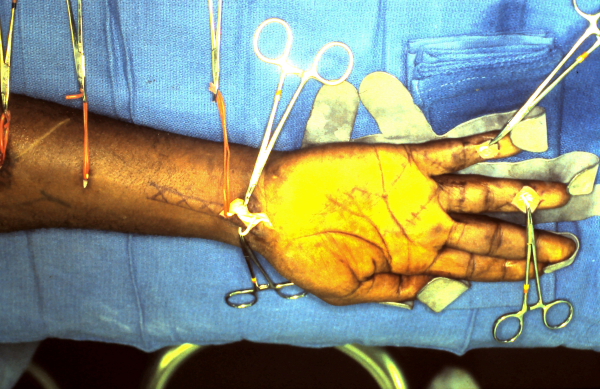
 Pre-operative full flexion before second stage tendon grafting.
Pre-operative full flexion before second stage tendon grafting.
 Palmaris longus is marked out for one tendon graft, likely the little finger since it will require a shorter graft than the ring finger. The plantaris tendon or second toe extensor will be harvested for the ring finger.
Palmaris longus is marked out for one tendon graft, likely the little finger since it will require a shorter graft than the ring finger. The plantaris tendon or second toe extensor will be harvested for the ring finger.
 Harvesting the palmaris longus tendon. Also, isloation of the distal end of the silicone tendon spacer and distal profundus tendon stump is achieved through a small Brunner incision at the distal interphalangeal joint.
Harvesting the palmaris longus tendon. Also, isloation of the distal end of the silicone tendon spacer and distal profundus tendon stump is achieved through a small Brunner incision at the distal interphalangeal joint.
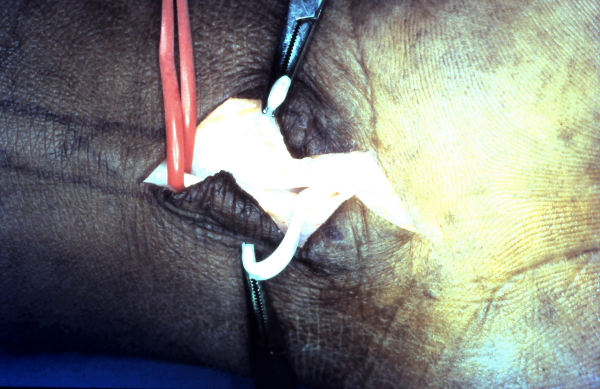
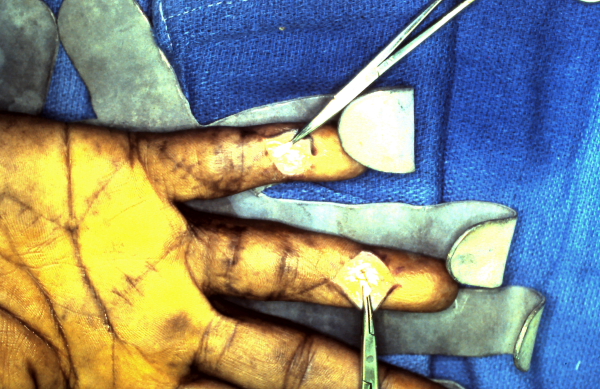 Silicone spacer and profundus stumps visulalized.
Silicone spacer and profundus stumps visulalized.
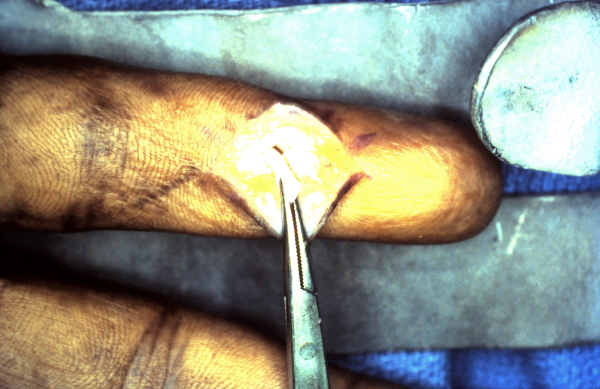 Close up of distal end of the silicone tendon spacer creating a new synovial tendon sheath.
Close up of distal end of the silicone tendon spacer creating a new synovial tendon sheath.
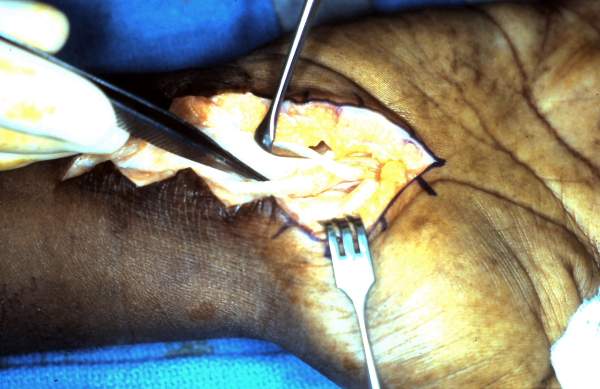
 The proximal ends of the silicone tendon spacers are identified and the tendon grafts are sutured to them so they can be withdrawn at the distal interphalangeal joint level passing the tendon grafts in place of the spacer in the new synovial lined flexor sheath.
The proximal ends of the silicone tendon spacers are identified and the tendon grafts are sutured to them so they can be withdrawn at the distal interphalangeal joint level passing the tendon grafts in place of the spacer in the new synovial lined flexor sheath.
 The grafts are attached to the distal phalanx and profundus tendon stumps first. Then the proximal tendon junctures are made between the grafts and the profundus tendons of the index and middle fingers as the proximal motor at appropriate tension to allow full digital flexion of all digits.
The grafts are attached to the distal phalanx and profundus tendon stumps first. Then the proximal tendon junctures are made between the grafts and the profundus tendons of the index and middle fingers as the proximal motor at appropriate tension to allow full digital flexion of all digits.
 Natural post operative resting cascade.
Natural post operative resting cascade.
 Active flextion is started after 6 weeks of dynamic flexion exercises. Blocking technique demonstrate profundus tendon function to the ring and little fingers.
Active flextion is started after 6 weeks of dynamic flexion exercises. Blocking technique demonstrate profundus tendon function to the ring and little fingers.
 Active flexion demonstrated in the relatively early post operative period. Hooks are still on the nails for dynamic flexion exercises.
Active flexion demonstrated in the relatively early post operative period. Hooks are still on the nails for dynamic flexion exercises.